Three Frameworks That Make Preventable Hospital Harm Visible, Prosecutable, and Fixable
Applying the Continuity Risk Framework, Clinical Moral Distress Scaffolding, and COVE-F

Part 3 of 5 - Paid. Parts 1 and 2 established the case and mapped the system breakdowns. Part 1 covered the clinical events: admission to a non-capable facility, transfer delayed 3-4 days, arrest, unsafe post-code staffing, transport mismatch, intensivist cancellation on grounds of instability that arose during the delay. Part 2 mapped the structural contributors: recognition failures, handoff collapse, policy deviations, regulatory gaps, and the institutional conditions that made each failure sustainable. This post applies three analytic frameworks to the case. Together, they move the analysis from description to proof architecture.
SECTION V – ANALYTIC FRAMEWORKS
Framework Integration: Continuity Risk, Moral Distress, and COVE F
Three analytic frameworks highlight how harm in this case can be understood as a structural phenomenon:
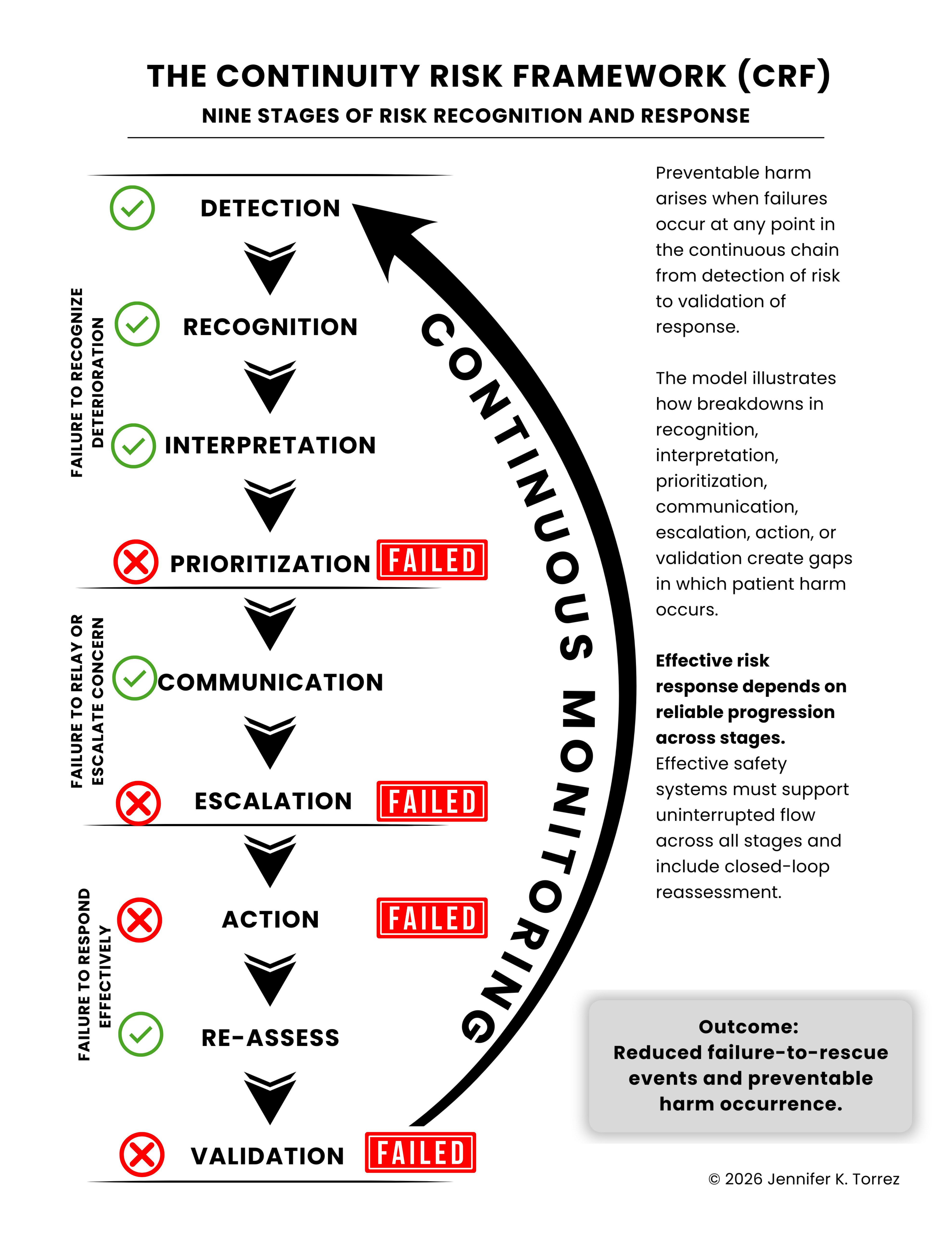
Continuity Risk Framework (CRF)
CRF describes nine stages required for risk to be recognized and acted upon effectively: detection, recognition, interpretation, prioritization, communication, escalation, action, reassessment, and validation. In this case, delays in arranging transfer from a non‑capable facility, failure to implement 1:1 post‑arrest care, and absence of in‑person specialist response suggest failures in prioritization, escalation, action, and validation.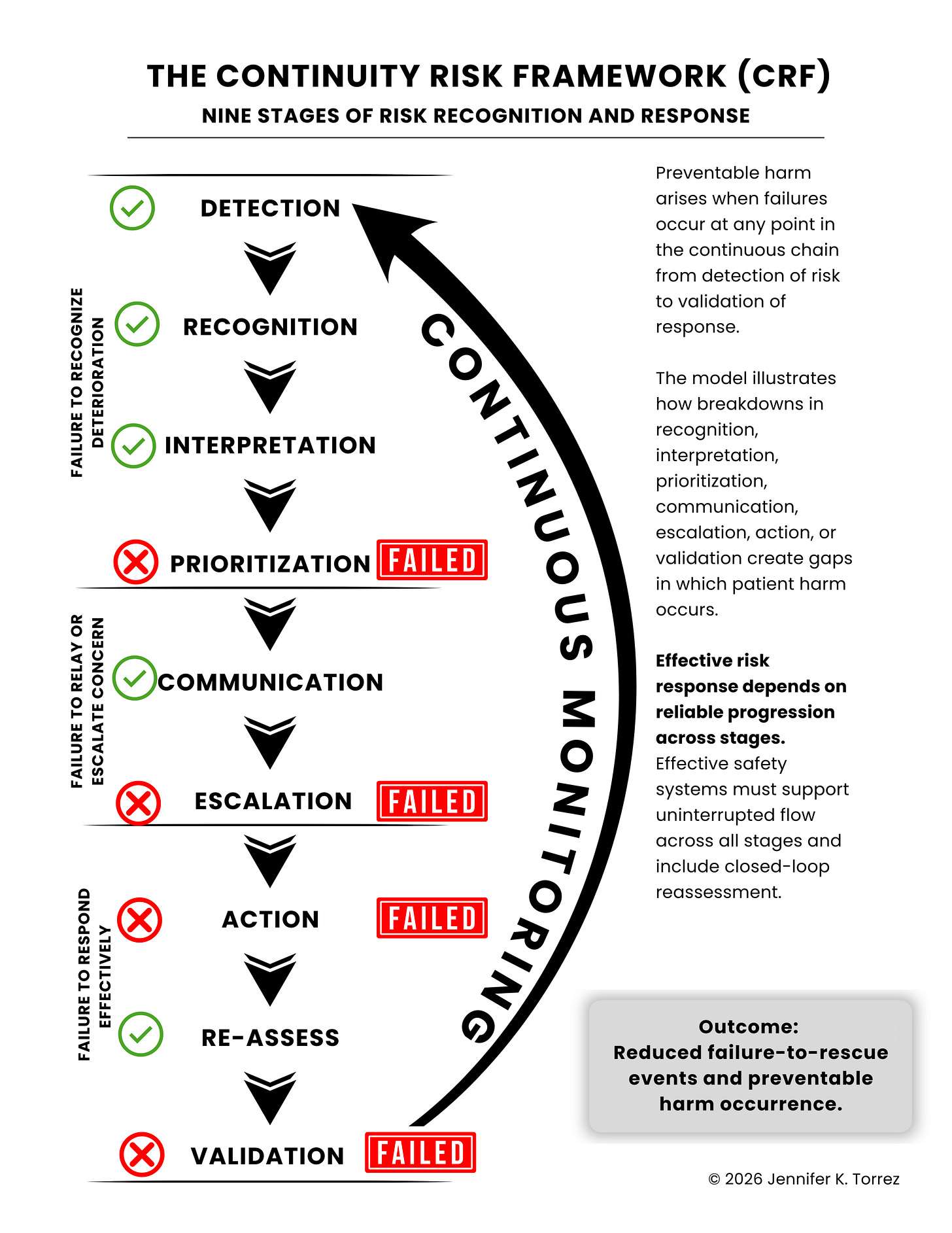
CRF identifies where the risk pathway broke. The next two frameworks, CMDS and COVE-F, explain why: the institutional mechanisms that suppressed intervention and the structural conditions that made preventable harm an operating feature, not an aberration. Table 1 integrates all three.